Abdominal Aortic Aneurysm (AAA)
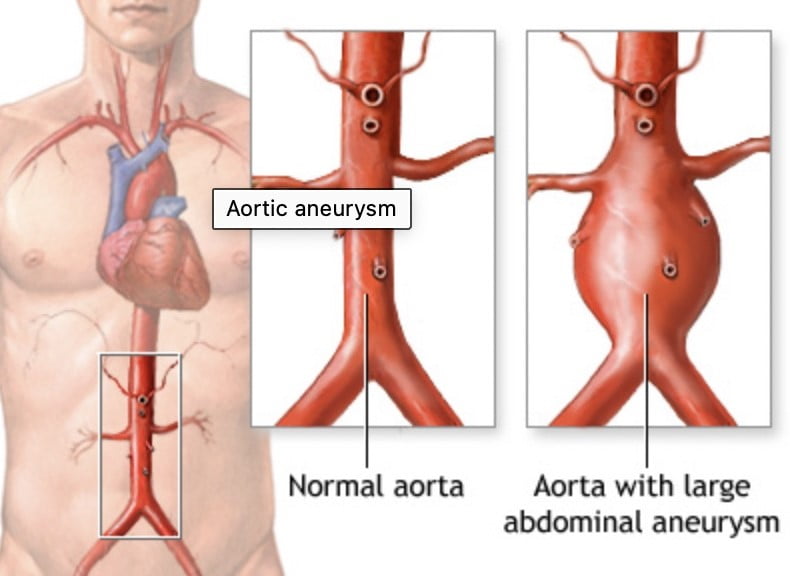
An abdominal aortic aneurysm occurs in the lower part of the aorta, your body’s major artery. The aorta is roughly the diameter of a garden hose and it pumps blood away from your heart. An aneurysm is an abnormal enlargement of your native artery caused by a weakening of its wall. This weakened area may grow into a large unstable dilated area which is called an aneurysm.
There are several known risk factors for abdominal aortic aneurysm including:
- Family history of aneurysm
- Being male
- Being >65 yrs age
- History smoking
- High blood pressure
- Hardening of the arteries/atherosclerosis
- High cholesterol
- Having a connective tissue disease like Marfans syndrome or Ehlers Danlos
Smoking is the no.1 factor associated with abdominal aortic aneurysm growth. If you have been diagnosed with an aneurysm, you should quit smoking immediately.
What happens if I am diagnosed with an AAA?
Abdominal aorta aneurysms are diagnosed at different sizes and are often picked up incidentally on CT imaging for other health issues. They grow at different rates and can have symptoms or be asymptomatic.
Think of your aorta like a balloon… as a balloon expands, its wall gets thinner… until it gets to a certain point and it bursts. If this happens with an aorta- there is massive internal bleeding, severe back or abdominal pain, collapse & death.
The aorta rupture rates are associated with AAA larger than 5cm, this exponentially increases as the AAA size increases. There is not a ‘one size fits all so you will be evaluated, educated, optimised & kept under regular surveillance by Dr O’Donnell. Some aneurysms may never get to the size where they need surgery.
- Operating on aneurysms is not without risk so surgery should only be performed when any operative risk is outweighed by benefit for you the patient. Dr O’Donnell will explain all these factors to you, specific to your individual situation and aneurysm. With diameters <5cm AAA patients rarely have complications.
- If you have an AAA, your direct family members are at four times greater risk of developing one. They should be screened once they reach 60 years of age. You should let them know this.
If you have an AAA, and experience new back or abdominal pain, go to the nearest emergency department. Notify them that you have a AAA when you arrive. This is because your aneurysm may be rapidly expanding or have ruptured. It is a medical emergency.
Abdominal aortic aneurysm surgery
Having an aneurysm repaired is a large operation. It does not matter if the procedure is endovascular or a traditional open bypass repair. Surgery carries risks that must be considered when assessing if a patient is medically fit to survive surgery without major complications. The patient’s medical history, current medications, and any other health conditions should be discussed with the medical team prior to any aneurysm repair.
A physical examination and imaging studies will be done to help determine the size and location of the aneurysm, as well as any other related medical conditions. Depending on the size and the patient’s overall health, the team will decide if surgery is the best option.
If a patient is deemed medically fit for surgery, the doctors may opt for endovascular repair or open bypass. Both procedures have their advantages and disadvantages and the team will discuss these with the patient to help decide on the best course of action.
- Endovascular aortic aneurysm repair (EVAR)
EVAR involves inserting a graft within the aneurysm through small incisions in the groins. Dr O’Donnell uses wires, contrast dye and X Ray machine to guide the graft into the correct position.
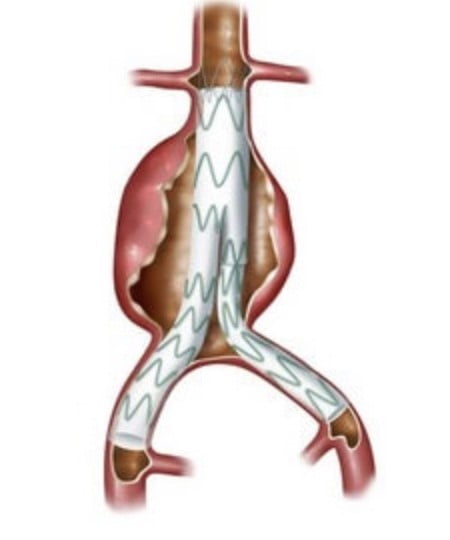
The advantage is there is no abdominal surgery and less time spent in hospital. Not every patient is suitable for this technique and Dr O’Donnell will carefully assess your imaging for this reason. Average hospital stay is 2-3 days after surgery and you will need long term follow up ultrasound or CT imaging to ensure the stent graft seal is maintained effectively. If issues arise with the stent graft, the vast majority can be dealt with minimally invasive techniques.
people with high blood
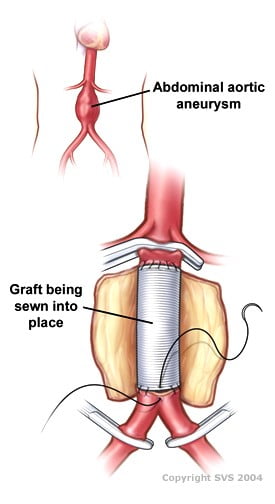
- Open aneurysm repair
Open aneurysm repair is often reserved for cases not suitable for endovascular options or in younger, fit patients. This is because it places the body under much greater stress than the minimally invasive approach.
This is the traditional treatment of aneurysms, involving open surgery to replace the aneurysm sac with a synthetic blood vessel/graft. A large incision is made in the abdomen. The blood vessels above and below the aneurysm are clamped. The aneurysm is then opened. Any blood clot in the aneurysm is removed and bleeding vessels are controlled. The synthetic graft is stitched into place with permanent sutures.
Post operative complication & death rates are higher as it is more invasive; hospital stays & post op recovery is also significantly longer. It is a good durable option for certain patients.
Australia & New Zealand Society of Vascular Surgery AAA advice